|
1. Female Urinary Incontinence
This is defined as a condition in which a demonstrable involuntary loss of urine has become a social or hygienic problem. Fifty percent of women will be affected at some point in their lives. It occurs in 36% of women aged between 35 and 50 years.
1.1 Genuine Stress Incontinence
GSI is a demonstrable involuntary loss of urine when intravesical pressure exceeds the maximum urethral pressure due to an increase in intra-abdominal pressure in the absence of a detrusor contraction. Risk factors include:
- family history (Musshkat et al. 1996)
- age (menopause - reduction in vaginal collagen, Jackson et al. 1996)
- obesity
- vaginal delivery, multiparity (>5) (Wilson et al. 1996)
GSI can be caused by either bladder neck/ urethral hypermobility or intrinsic sphincter deficiency.
Bladder neck/ urethral hypermobility is shown by: a positive 'Q tip' test and upward movement of the urethral axis by more than 30°, a positive Bonney test, valsalva leak point pressure (VLPP) of greater than 90 cm of water (McGuire et al. 1993) and maximum urethral closure pressure (MUCP) greater than 50 cm of water.
Intrinsic sphincter deficiency is shown by: a VLPP of less than 60 cm water, a MUCP of less than 20 cm of water which is associated with failure of colposuspension (Sand et al. 1987) and an open bladder neck in the absence of raised abdominal pressure (seen on video UDS)
Management
- Conservative
- Oestrogen
- Behavioural therapy
- Other
- Surgical
- Urethral hypermobility
- Intrinsic sphincter deficiency
Conservative management
Conservative management with oestrogen results in no objective improvement in continence (Fantl et al. 1994) but the outcome may improve after colposuspension (Byck et al. 1994). Oestrogen does improve sensory threshold however and increases MUCP by about 30%.
Behavioural therapy in the form of Kegel Pelvic floor exercises (Kegel 1948) increases the resting tone of periurethral and pelvic floor striated muscle (pubococcygeus) and increases the strength of reflex muscle contraction during increased intra-abdominal pressure. It has been shown to produce a 61- 85% improvement in symptoms and a 3-38% cure (de Kruif et al. 1996). Of these 65% are durable i.e. still continent after 5 years (Boet al. 1996).
Other therapies include the use of weighted vaginal cones which have shown a significant improvement in 70% of cases after 1 month (Peattie 1988) and transvaginal electrical stimulation which is reported to improve symptoms by 35-70% (Richardson 1996).
Surgical management - urethral hypermobility
Surgical techniques for urethral hypermobility (Blaivas & Olsson types I-II) include: Mid Urethral Sling, colposuspension, needle suspension, anterior colporraphy and laparoscopic colposuspension.
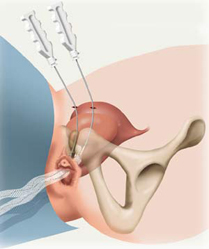
Mid Urethral Sling: Stress urinary incontinence surgery has been revolutionised by the arrival of tension free vaginal tape technique TVT . The use of SPARC (suprapubic arc) has opened up an interesting perspective simplifying the surgical procedure and making it more innocuous.
Suprapubic Arch sling (SPARC) is one such modification, where needles are driven from the suprapubic region to the vagina, in the opposite direction to TVT needles. The procedure is proposed to reduce the intra-operative complications of TVT, such as bladder perforation and retropubic bleeding, since the needles follow the curvature of the symphysis pubis, and theoretically avoiding important adjacent structures.
At 3.5-6 years the cure rate is 76-97% (Blaivas 1991; Morgan 1995; Weinberger 1995). However, there is no evidence for greater efficacy than colposuspension and in 25-32% of cases there is also secondary detrusor instability. In a retrospective study (Iosif 1983) that compared the sling with colposuspension, the cure rates were 70% and 95% respectively (P<0.001). In addition there are more complications with the sling and less than 5% maintain permanent urinary retention. All should be taught ISC preoperatively.
Results for the Burch colposuspension are better than those of the Marshall-Marchetti-Krantz (MMK) colposuspension, and there are also greater complications with MMK (e.g. BOO with secondary DI; osteitis pubis; sphincter injury).
Needle suspension has a 50-70% 1-year cure rate but only 20-30% remain dry at 10 years (Trockman et al. 1995). Similarly, anterior colporraphy has a 50-70% 1-year cure rate but with rapid diminishment and is inadequate as a primary treatment for GSI.
In comparative studies, Bergman et al. (1989) looked at the 1-year cure rates of colposuspension versus needle suspension versus anterior colporraphy in 342 patients and found that they were 87%, 67% and 70% respectively. But a smaller study (127 patients) by Elia & Bergman (1994) looking at 5-year cure rates found that the rates changed to 82%, 43% and 37% for colposuspension versus needle suspension versus anterior colporraphy respectively.
Laparoscopic colposuspension has a longer operating time and may also have reduced efficacy. In a study of 60 patients comparing open versus laparoscopic colposuspension, the 1-year cure rate was 97% and 73% (P=0.03) respectively (Burton 1994).
Surgical management - intrinsic sphincter deficiency
Surgical techniques for intrinsic sphincter deficiency (ISD) (Blaivas & Olssen type III) include suburethral sling procedure, urethral bulking and artificial urinary sphincter (AUS). The failure of these multiple anti-incontinence procedures is associated with a 75% incidence of ISD (McGuire 1981).
The objective of the suburethral sling procedure is to restore sufficient outlet resistance whilst avoiding obstruction. It was first described by Goebell in 1910 and since then numerous techniques have been described.
Slings can be either organic or synthetic but prosthetic slings have a higher incidence of erosion and fistula formation (up to 14%).
Urethral bulking increases urethral resistance (for review see Williams 1997) and can be carried out by either transurethral or periurethral injection under local anaesthetic. However, the volume injected is not predictive of the outcome. There are good short-term results with a cure or improvement in 70-90%, but long-term results are disappointing with only an 18-60% success rate at 3 years.
One problem is the migration potential of the particles in the bulking medium. Particles of greater than 80 µm cannot be phogocytosed which reduces the migration potential. This was first described using PTFE by Politano (1974) where 90% of the particles are less than 40 µm. Associated complications with PTFE were urethral fibrosis (10%), granuloma balls (15%), abscesses and diverticula. It is not recommended for use in the urethra.
Other bulking media include autologous adipose cells which can be subject to resorption. There have been some small studies with a short follow-up of 1 year which have shown a 21-23% cure (Blaivas 1994; Gonzalez 1991). Bovine collagen can also be prone to resorption and may cause an allergic reaction in 1-3%. Approximately 40% of patients require multiple injections (Appell 1994)but, at 1 year, there is a 20-50% cure with a 20-60% improvement (Monga 1995; Moore 1995).
Silicone (macroplastique) is composed of particles between 100-600 µm. The long-term risks of distant migration resulting in possible connective tissue disorders are unknown. In the short-term (<1 year) the cure is 82-95% (Buckley 1992; Sheriff 1994). The maximum follow-up reported is 17 months. This shows a 70% cure and 10% improved in 144 patients (Chaliha 1995).
Artificial urinary sphincter (AUS) is reserved for women with ISD and an acontractile detrusor and who cannot perform ISC (Hadley 1995). It can be performed by either an abdominal or transvaginal insertion. At 5 years 94% are still dry compared to 81% with sling (Mark & Webster 1994).
1.2 Urge Incontinence
This is defined as the leakage of urine accompanied by a strong desire to void. When it is associated with documented detrusor instability it is known as detrusor instability incontinence. The majority of patients are idiopathic (2% of MS patients present only with detrusor hyperreflexia, Miller 1965). The urodynamics show symptomatic phasic waves (pdet>5 cm H20) on filling spontaneously or on provocation, causing urgency or urge incontinence in the absence of a raised pabd. They may also show a raised UPP and flow rate.
Management
- Conservative
- Dietary advice/bladder drill
- Electrical stimulation
- Medical
- Anticholinergic agents
- Musculotropic relaxants
- Others
- Surgical
- Augmentation enterocytoplasty
- Detrusor myectomy
- Denervation
Conservative management
Conservative management includes advice on avoiding caffeine and reducing fluid intake and electrical stimulation. Stimulation of the non-muscular afferent somatic fibres of the pudendal nerves can inhibit unstable contractions. Electrical stimulation can be given transvaginally, perineally or via sacral neuromodulation.
Transvaginal RCT electrical stimulation (20 Hz) for 8 weeks has been shown to produce a 38-49% cure on UDS testing (Sand 1996).
Perineal electrical stimulation with TENS is also successful. A comparison TENS placed over S2/3 dermatomes versus temporary S3 neuromodulation produced similar subjective and objective results (Hasan 1996). Madersbacher (1995) used TENS and showed an increase in maximum cystometric capacity and a reduction in diurnal frequency.
Sacral neuromodulation acts primarily by activation of nonmuscular pudendal somatic afferent nerve fibres that inhibit pelvic parasympathetic motor nerves supplying the bladder through interneurones. It is beneficial for controlling refractory detrusor instability and the S3 nerve root is the most practical for chronic electrical stimulation.
After a percutaneous nerve evaluation a percutaneous test electrode is placed in the S3 foramina for 4-7 days. If there is a greater than 50% improvement in continence (usually 60-70% of those tested) a permanent implant is considered. This consists of the foramen electrode, an extension cable and a pulse generator.
In general there is a poor response in males to this technique particularly when the first unstable wave occurs at less than 200 ml or when capacity is less than 250 ml and there is a low initial mental component of 'Short form 36'.
Overall, sacral neuromodulation has a long-term success rate of 50-60% at 3-4 years (Bosch 1996) and early results with MS patients are promising (Bosch 1996). There are QOL benefits but generally it is not cost effective, for example the pulse generator has a finite life. There can also be complications in the form of electrode dislocation (6%), device explant (6-33%) and pulse generator repositioning (1.5%).
Medical management
This includes the use of anticholinergic agents, musculotropic relaxants and others such as tricyclic antidepressants.
Anticholinergic agents
Non-selective antimuscurinic agents (e.g. propantheline) result in partial inhibition with poor uroselectivity causing unwanted side effects (dry mouth, nausea/reflux, drowsiness, tachycardia, constipation, blurred vision and urinary retention). However, there are less side effects with some M3 receptor antagonists such as tolterodine (non-selective) (Abrams 1998) and darifenacin (selective).
Musculotropic relaxants
Musculotropic relaxants such as oxybutinin have combined anticholinergic and local anaesthetic properties. Results so far have shown 60-70% objective and subjective improvements respectively. Side effects can be reduced however if the dose titrated is 2.5 mg bd.
Other
Other methods such as oestrogens have been used to reduce urinary storage symptoms in post-menapausal women (Walter 1978) but they do not stabilise detrusor activity. Desmopressin/Tricyclic antidepressants (imipramine) are useful in nocturia and nocturnal eneuresis.
Surgical Management
This is reserved for those with intolerable symptoms who have failed conservative therapy. There are three types of surgery: augmentation enterocytoplasty, detrusor myectomy and denervation.
Augmentation enterocytoplasty
Clam ileocystoplasty is the most commonly used method. A 20 cm segment of the distal ileum is opened on its antimesenteric border and anastamosed to the bladder bi-valved in sagital or coronal plane, to form an acontractile pouch. This results in increased bladder capacity and dissipation of unstable detrusor contractions. The success rate is around 87-90% (Bramble 1982). However, neurological patients require close monitoring of ureteric (reflux) and renal function postoperatively, and there are also some complications. For example, 25% will require CISC, there can be an increase in mucous and recurrent UTI and, in 9 cases reported in the literature to date, malignancy with all patients requiring annual cystoscopy after 5 years.
Detrusor Myectomy
In this operation the bladder is filled to 250 cc. Following this an 8-12 cm diameter disc of detrusor muscle is dissected from the bladder dome together with an omental patch to 'bare' urothelium in order to create an acontractile diverticulum. Early 1-year results are encouraging so far with a 70% success rate in idiopathic DI (Swami 1998). Long-term results are unknown.
Denervation
This is carried out using a modified Ingleman-Sundberg technique: an inverted U is cut in the anterior vaginal wall and dissected of bladder which causes local denervation. There is a 64% cure or significant improvement.
1.3 References
Abrams 1998 Br. J. Urol. 81, 801-810
Appell 1994 J. Urol. 151, 418A
Bergman et al. 1989. Am. J. Obstet. Gynecol. 161, 97-101
Black & Downs 1996. Br. J. Urol. 78, 497-510
Blaivas 1991 J. Urol. 145, 1214-1218
Blaivas 1994 J. Urol. 151, 419A
Bosch 1996 J. Urol. 155, 594A
Bosch 1996 Lancet 348, 717-719
Bramble 1982 Br. J. Urol. 54, 693-696
Buckley 1992 J. Urol. 147, 280A
Burton 1994 Neurourol. Urodynam. 4, 497-498
Byck et al. 1994. Am. J. Obstet. Gynecol. 17, 1460-1462
Chaliha 1995 Br. J. Urol. 76, 151-155
de Kruif et al. 1996. Physiotherapy 82, 107-113
Elia & Bergman 1994 Neurourol. Urodynam. 4, 498-500
Fantl et al. 1994 Obstet. Gynecol. 83, 12-18
Gonzalez 1991 Arch. Esp. Urol. 44, 595
Hadley 1995 J. Urol. 153, 432A
Hasan 1996 J. Urol. 155, 2005-2011
Iosif 1983 Arch. Gynecol. 233, 93-100
Jackson et al. 1996 Br. J. Urol. 77, 805-812
Jackson et al. 1996 Lancet 357, 1658-1661
Kegel 1948 Am. J. Obstet. Gynecol. 36, 238
Madersbacher 1995 Neurourol. Urodyn. 14, 501-502
Mark & Webster 1994 J. Urol. 151, 420A
McGuire 1981 Prog. Clin. Biol. Res. 78, 351
McGuire et al. 1993 J. Urol. 150, 1452
Miller 1965 BMJ 1, 1265
Monga 1995 Br. J. Urol. 76, 156
Moore 1995 Br. J. Urol. 75, 359
Morgan 1995 J. Urol. 154, 1214-1218
Musshkat et al. 1996 Am. J. Obstet. Gynecol. 174, 617-619
Peattie 1988 Br. J.Obstet. Gynecol. 85, 1049
Politano 1974 J. Urol. 111, 180
Richardson 1996 Urology 129, 110-8
Sand 1996 Obstet. Gynecol. 88, 757-760
Sand et al. 1987 Gynec. 69, 399
Sheriff 1994 J. Urol. 151, 419A
Swami 1998 Br. J. Urol. 81, 68-72
Trockman et al. 1995 J. Urol. 154, 1841-1847
Walter 1978 Urology 33, 135
Weinberger 1995 Obstet. Gynecol. 86, 92-96
Williams 1997 European Urology Update Series 6, 66-71
Wilson et al. 1996 Br J. Obstet. Gynaecol. 103, 154 |